Clinical Vignette
This 66-year-old female presents with atypical cells on peripheral blood smear. A peripheral whole blood sample is submitted for flow cytometric immunophenotyping using ClearLLab 10C Panels.
Flow Cytometric Immunophenotyping
T Cell Tube
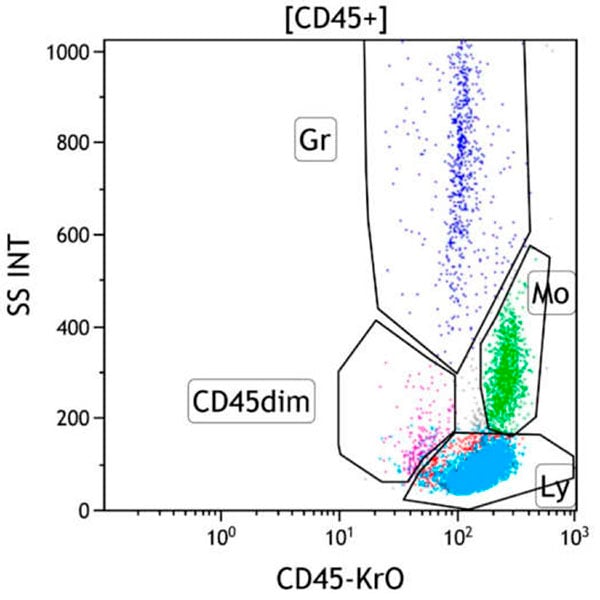
Figure 1. This CD45 vs Side Scatter dot plot shows events in the CD45+ gate. This dot plot permits distinction of several white cell populations typically found in peripheral blood, bone marrow, and lymph node samples, including lymphocytes (Gate Ly, red/aqua), monocytes (Gate Mo, green), and granulocytes (Gate Gr, blue). The CD45 dim gate (purple) covers the area typically occupied by myeloblasts and immature B cells. Basophils, plasmacytoid dendritic cells, plasma cells and NK cells may also fall in this area. By applying different colors to the events comprised by each gate, the various populations may be followed throughout the analysis. Note the relatively increased number of lymphocytes (red/aqua).
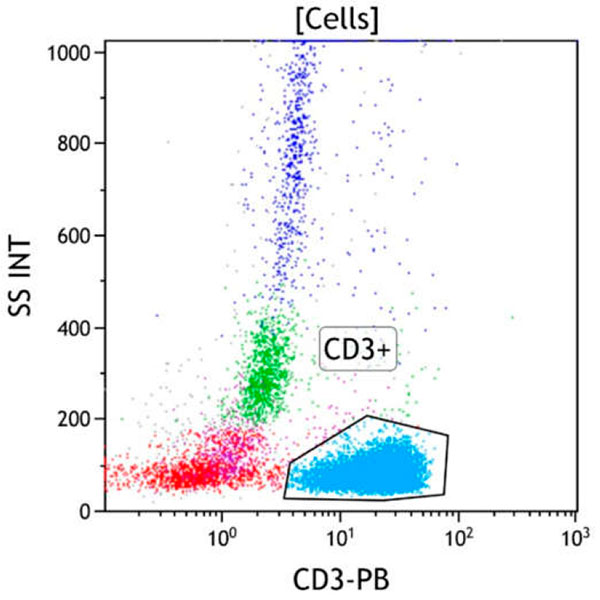
Figure 2. This CD3 vs Side Scatter dot plot shows all viable cells. The CD3+ gate identifies cells with surface CD3 expression (aqua). CD3 is highly specific for T cells, being expressed only on the surface of mature T cells and later stage immature T cells. These cells typically have low to moderate side scatter. Most lymphocytes are CD3 positive T cells (aqua).
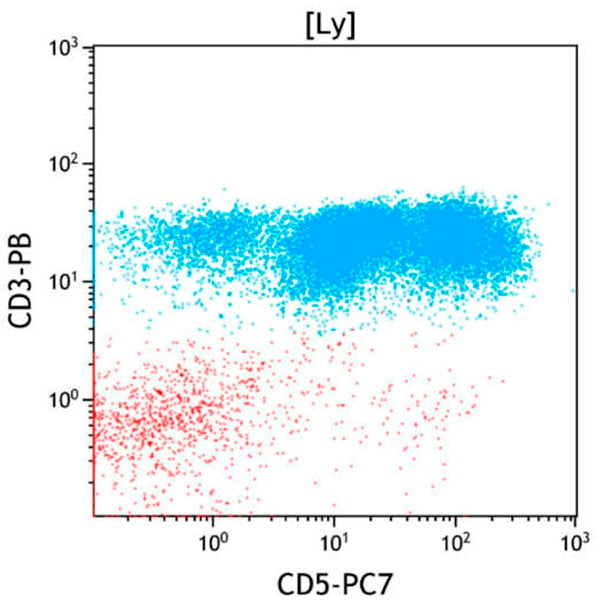
Figure 3. This CD5 vs CD3 dot plot shows all cells in the Lymphocyte gate (Ly). CD3 and CD5 are coexpressed on most mature T cells (aqua), although a small subset of cytotoxic T cells having a large granular lymphocyte morphology often shows reduced to absent expression of CD5. CD5 is not expressed on most NK cells (red). CD5 expression is variably decreased on a subset of T cells.
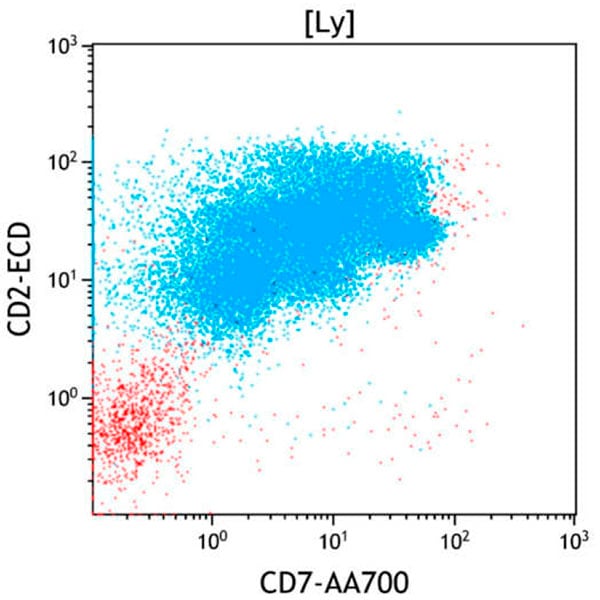
Figure 4. This CD7 vs CD2 dot plot shows all cells in the Lymphocyte gate (Ly). CD2 and CD7 are coexpressed on the large majority of mature T cells (aqua) and NK cells (red). CD2 and CD7 are variably decreased on a subset of T cells.
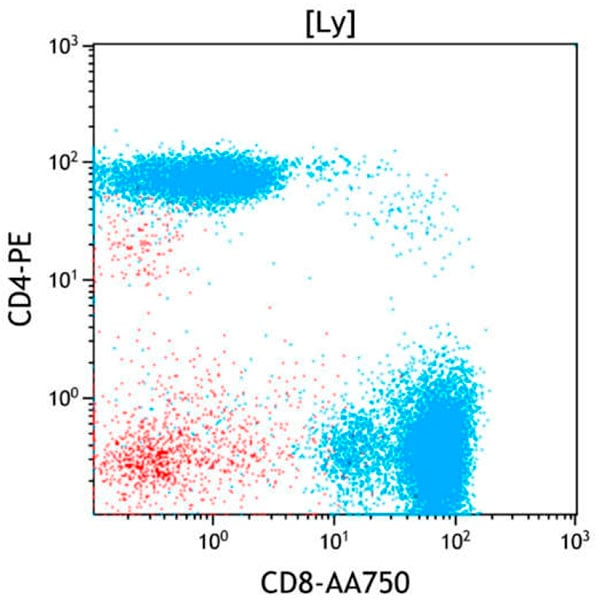
Figure 5. This CD8 vs CD4 dot plot shows all cells in the lymphocyte gate (Ly). CD3 positive T cells (aqua) contain CD4 positive (helper) and CD8 positive (cytotoxic) subsets. CD4 positive T cells usually outnumber CD8 positive T cells with a CD4:CD8 ratio of 1:1 to 4:1 in peripheral blood. Occasional CD4 and CD8 double negative or double positive T cells are also present. The double negative T cells typically consist mostly of gamma/delta T cells. Of note, the CD4 positive but CD3 negative cells (red, middle left) are monocytes included in the lymphocyte gate. It demonstrates that CD45 vs Side scatter gating alone does not allow pure lymphocyte identification. CD8-positive T-cells are proportionally increased.
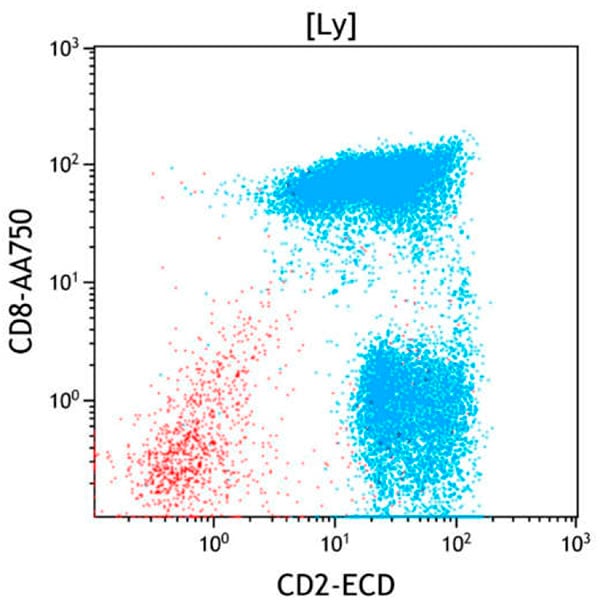
Figure 6. This CD2 vs CD8 dot plot shows all cells in the lymphocyte gate (Ly). Compared to the CD8-negative T cells (blue, lower right), a large subset of CD8 positive T cells (blue, upper right) show aberrantly decreased CD2 expression.
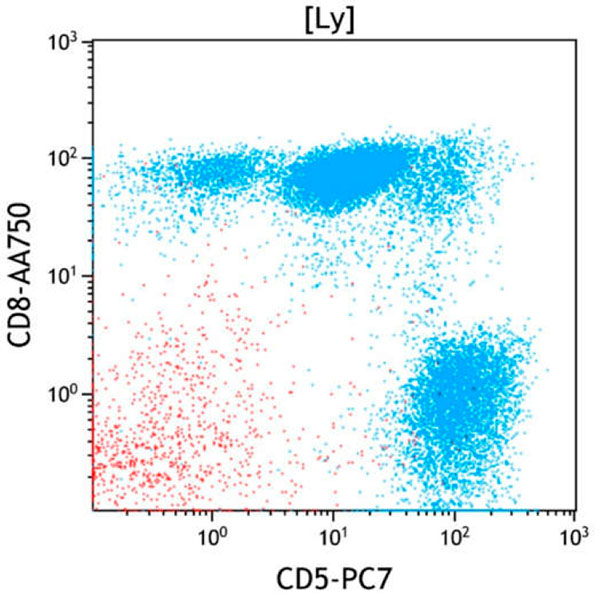
Figure 7. This CD5 vs CD8 dot plot shows all cells in the lymphocyte gate (Ly). Compared to the CD8-negative T cells (blue, lower right), a large subset of CD8 positive T cells (blue, upper) show aberrantly decreased CD5 expression.
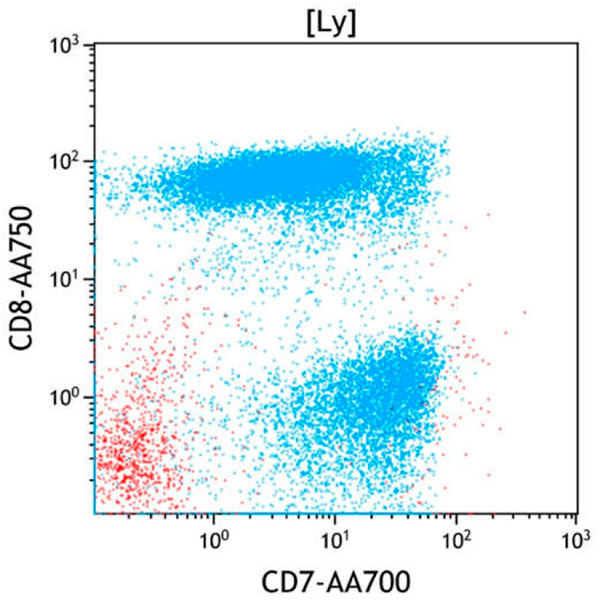
Figure 8. This CD7 vs CD8 dot plot shows all cells in the lymphocyte gate (Ly). Compared to the CD8-negative T cells (blue, lower right), a large subset of CD8 positive T cells (blue, upper) show aberrantly decreased CD7 expression.
To view all flow cytometric dot plots, download the case in PDF format below
Results of Flow Cytometric Immunophenotyping
Flow cytometric immunophenotyping identifies a phenotypically distinct population of cells with expression of variable CD2, intermediate CD3, variable CD5, variable CD7, bright CD8, bright CD45 and low CD56 on a subset. This population also likely expresses CD16 on a subset. Compared with normal mature T cells, the decreased expression of CD2, CD5 and CD7 with increased CD16 and CD56 is aberrant.
The immunophenotype of the abnormal population is consistent with expanded abnormal large granular lymphocytes of T cell type. In the appropriate clinical context of prolonged cytopenias without other explanation, this finding would be consistent with a large granular lymphoproliferative disorder.